
Table of Contents
Introduction
“Who will NOT require hospitalization in COVID-19?” Is there a simple number that can be used to identify which of the COVID-19 infected patients will easily recover sitting at home?
A recently conducted survey shows that this is a burning issue in today’s pandemic haunting everyone.
It’s clear that COVID-19 infection can’t be really stopped. One wave after the other have been raging across the world and will continue. Millions have died. It’s really terrifying. But we also know that majority recover easily. Only a few require hospitalization. Despite this fact, each wave of this pandemic overloads the existing healthcare systems with hospitals running out of beds.
At present there is really no way to predict right at the start which patient, infected with COVID-19, will develop complications. If such prediction is made possible, we shall be able to focus our resources on only those who really need, and decisively intervene at a very early stage- while other patients might just relax at their homes. Such early intervention, focused on the ones who will eventually develop complications on COVID-19 infection, will significantly reduce hospitalization rate and mortality. But is there a way to accurately predict which patient will deteriorate and will require such early intervention?
This is exactly what we will try to answer. Let’s see if we succeed.

This post is the third part of the four-parts series that intends to eventually show how we can easily predict outcomes of COVID-19 infected patient at a very early stage.
(If you haven’t read the first two parts, I will strongly recommend doing so. For the first part, click HERE. For the second part, click HERE.)
What will we learn in this post?
In the first part of this series we focused on understanding why it is more important to predict who will die in COVID-19 rather than just focusing on prevention and treatment of all. We also explored how vaccines and anti- viral drugs might not help in completely wiping off this pandemic. In the second part, we explored the basics of immunology behind “COVID-19 induced cytokine storm”, which is real of cause of death in majority.
In this post:
- We will explore how a healthy immune system prevents cytokine storm in majority of the patients with COVID-19 infection.
- We will also thoroughly investigate the defects in immune system of few people that make them unlucky enough to suffer from this horrific complication.
This journey of scientific exploration will be done using very simple language such that every reader, irrespective of his/her background will easily understand.
Aggression Is a Weapon of the Weak!

Cytokine storm ideally must not happen, and actually they don’t in majority of the cases. Occurrence of cytokine storm is in stark contrast with the first principle of immune system- it’s our immune systems duty to ensure foreign antigens are destroyed without its own cells. Cytokine storm occurs when this differentiation is completely lost- when immune system decides that killing virus is the most important aim, even at the cost of the organism’s own life. This is not a sign of strength- this is a sign of immaturity. And immature excessive use of power blindly is a definite weakness [1].
We already know that not all suffer from this weakness of blind and senseless immune system. It has been repeatedly documented that old age, co-morbidities such as diabetes, heart diseases etc make a Covid-19 patient more likely of developing cytokine storm compared to young and healthy patients [2][3]. In the second part of this series, we understood how immune system interacts with Covid-19 virus. Now we will try to unravel the relationship of old age and comorbidities with cytokine storm. We will try to understand how old age and comorbidities can make immune system so edgy that when faced with COVID-19, it can lose its rigor; and then instead of being a noble administrator of justice it can become an uncontrollable monster. And in that attempt, we will also try to discover if there is a way to predict accurately whose immune system can sustain the rigor and whose immune system will adopt the route of devil!
Every cell Contributes To Defense
We need to start by emphasizing the fact that any event inside or around a living cell that is not conducive for efficient functioning of our systems is a threat [4]. The cause of threat can be internal or external. Irrespective of the source, the cause must be eliminated. And hence, each cell of our body is also a soldier. Each cell’s job is to efficiently do the assigned functions and try eliminating anything that doesn’t allow it to do its job perfectly. Going by the same rule, if any cell itself somehow becomes the cause of inefficiency it will quickly kill itself [5].
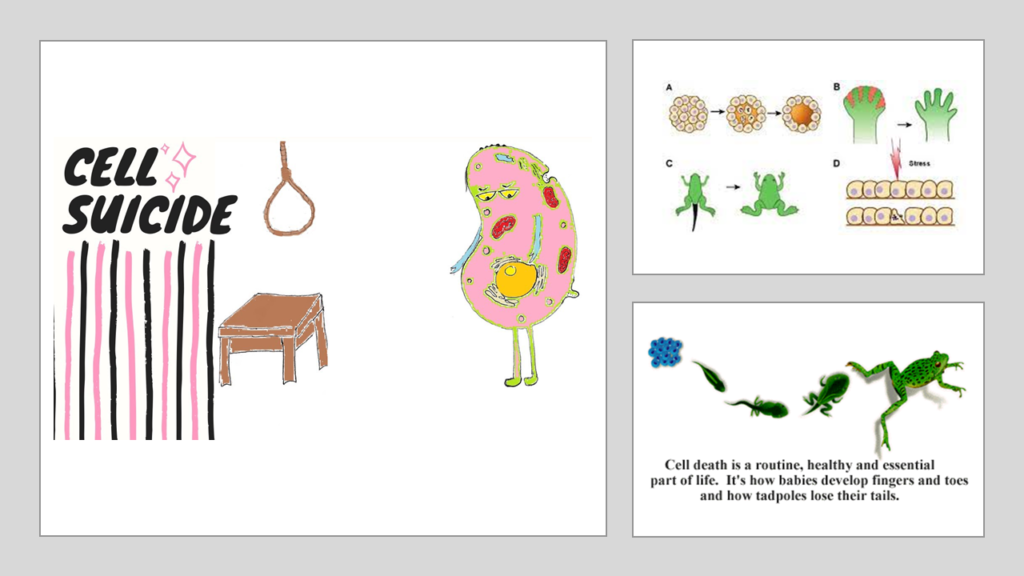
These are not some divine theoretical prophecies but are actually facts of life- the very facts that make life itself possible. A platelet is a cell found in blood. Its primary job is to act as a plumber. Whenever there is any leak in the plumbing system, aka the blood vessels, platelets rush to the site of leakage and repair the leak. But the same platelets also act as detectives to determine what was the cause of the leak and would step up and participate in mounting an attack in case the cause is detected [6]. When a platelet finds itself inefficient in performing its job as a plumber it commits suicide via a process called “apoptosis”[7]. Since such dead bodies left along the tracks unattended can obstruct functioning of other cells, such dead bodies are also identified as threats and are removed by cells of immune system.
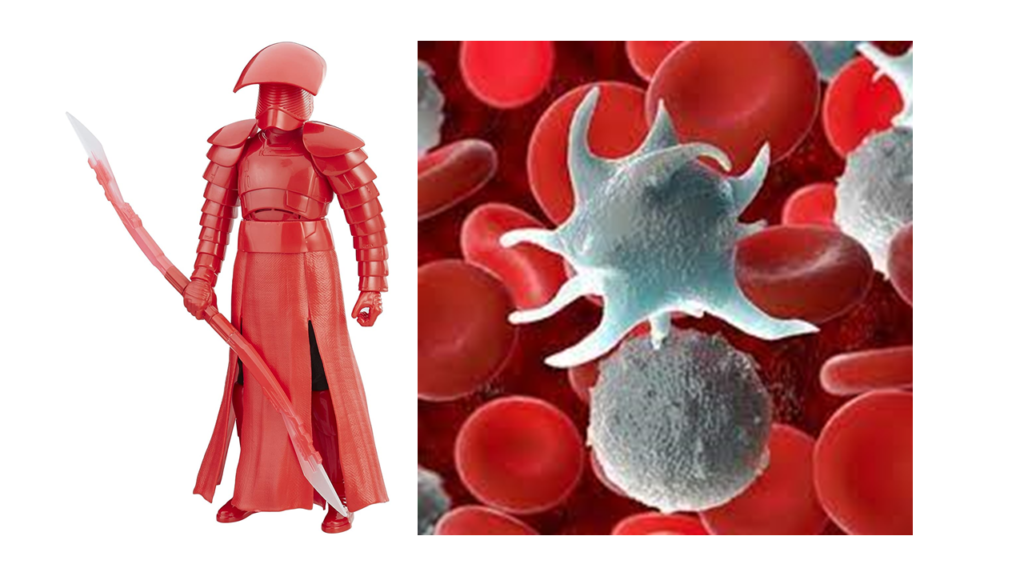
This description will quickly allow you to understand that while every cell has a respective primary function assigned, all cells contribute to the function of defense from any threat. This is necessary to tackle any threat immediately without waiting for the main forces to arrive. To reinforce this “rapid response” strategy, there are supporting cells such as neutrophils, mast cells etc. scattered across the body in ample amounts. Together, they constitute our primary line of defense called “Innate Immune System“. It needs to be acknowledged that in majority of the cases this is a sufficient response. Innate Immune System is powerful enough against most of the invaders.
Fallacies of Rapidity
However, this rapidly responsive innate immune system has its own fallacies. Because it’s rapid, the form of response is not tailor made. It is the same reason why service is faster in MacDonald’s and slower in Subway!
It’s not a trained “thought through” response. It’s akin to any immediate reaction someone might throw to any insulting action. Such reaction is never accurate, and many a times can be termed as immature in certain scenarios. It exactly in these scenarios where things can go massively wrong. We will discuss about such scenarios soon.

Thymus- The Training School
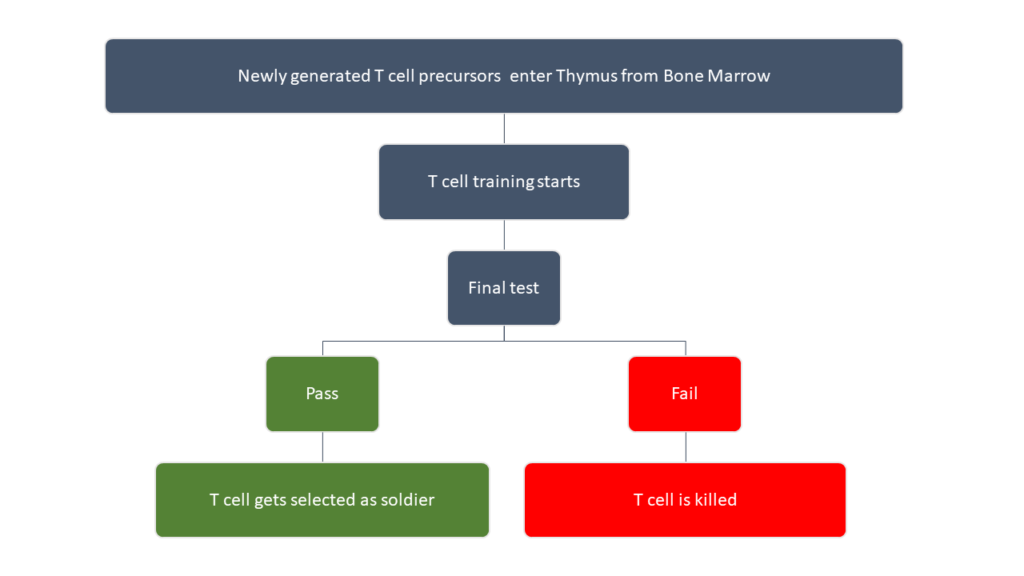
Now let’s turn our attention to those soldier cells that are born just to ensure accurate defense. They are the components of what we call as “Adaptive Immune System” [4]. Inside our body, the main components of blood are formed from few “mother cells” known as hemopoietic stem cells (HSCs) [8]. These HSCs are located mostly inside the bones in an area called “bone marrow”. Bone marrow can be imagined as nursing homes where HSCs give birth to soldier cells amongst many other cells. One such faction of soldier cells consists of what we call as T cells. These T cells, when they are born, are “immature”. Immaturity here means that these T cells are not trained. They potentially can’t differentiate between what is “self” and what is “non self”. Hence, they need to go to a school. This school is located in an organ called Thymus [9].
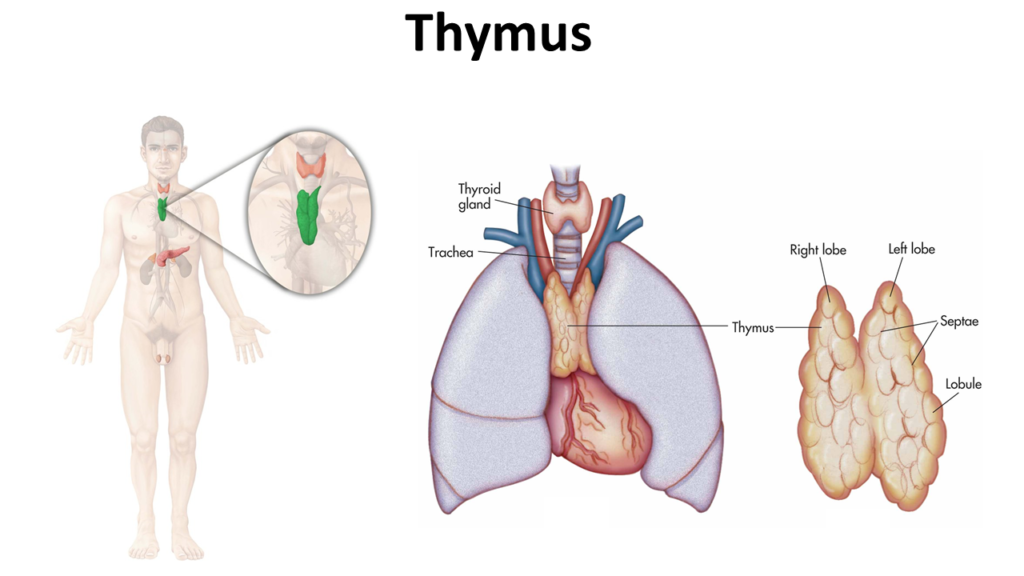
This is a butterfly shaped organ located beneath the chest bone. It is in thymus that these immature T cells arising from the wombs of HSCs get the real training of a true patriotic fighter. The T cells are now trained and “mature”.
Please note that I won’t be touching upon B cells for the sake of keeping things brief and simple. B cells are also very important players. But their story more or less is similar to that of T cells.
So, when innate immune system identifies any “threat” and reacts, the battle cry reaches these mature T cells as well via the APCs. APCs, we have noted earlier, act as bridge between innate and adaptive immune system [10]. At this point, it’s a good idea to quickly go back to the part two of this blog series and have a relook at what really happens. In nutshell, these trained T cells generate a mature response depending on the information received from the APCs. If the threat recognized is a false alarm, it swiftly silences the innate immune system [11]. If this silencing is not done, the only cells that will be killed by innate immune system will be our own healthy cells. It also trains the innate immune system to remember this “false alarm” so that such mistakes are not repeated. If it’s a real threat, these trained T cells are able to channelize all the forces and specifically target the cause while minimizing any “off target” impact.

And all this happens when immune system is healthy. But this healthy state of immune system is not permanent. With age, immune system keeps weakening. Many other factors can also weaken this immune system although the individual might be young.
When Supply Doesn’t Meet the Demand

When you are born, there is plenty of bone marrow. The size of thymus is quite significant. As you keep growing into adulthood, thymus size keeps increasing. But approximately by the time of puberty, this growth in size of thymus stops. And then it starts shrinking with age. Something similar happens with bone marrow as well.
In short, with age, the supply of trained T cells goes down.
You will now have to note another point- except few types of T cells (known as memory T cells), most of the T cells will die. They have to be replaced by new T cells. When you are young, these dying T cells get replaced by the new trained T cells supplied from thymus. But as age advances, the shrinking thymus slowly loses its capacity to develop and provide new trained T cells. Remember, even bone marrow (the primary producers of T cells) is also shrinking with age.
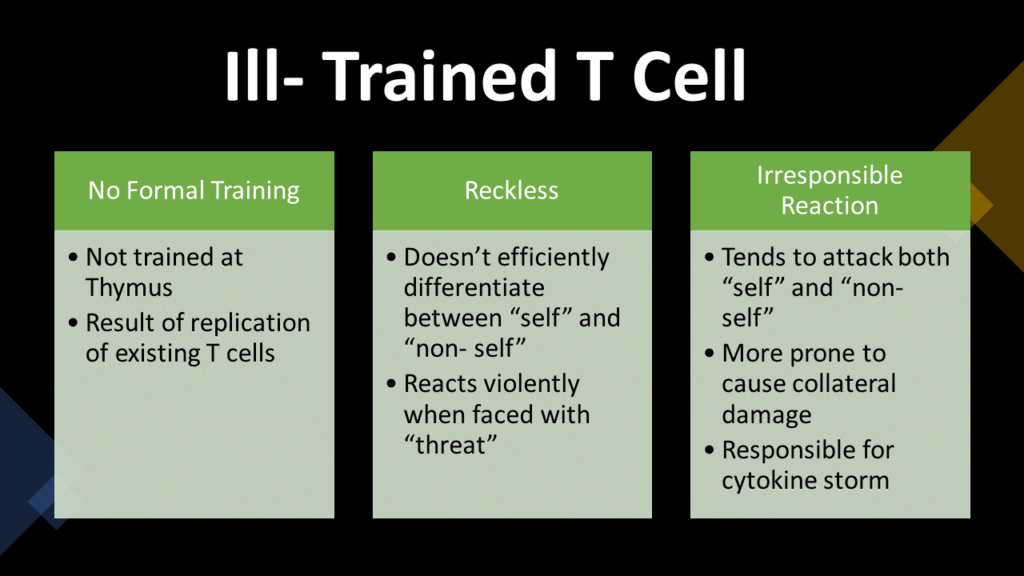
So, with advancing age, more and more T cells actually comes from multiplication of existing trained T cells. But these are children who have not gone to school. They have never been trained in thymus. Their parents were trained- but they are not. They still have learnt a few lessons from their parents. There are still few mature T cells around coming from Thymus. But slowly you have growing population of T cells who are not well trained. They don’t have enough discipline of differentiating between “self” and “non- self” [12].
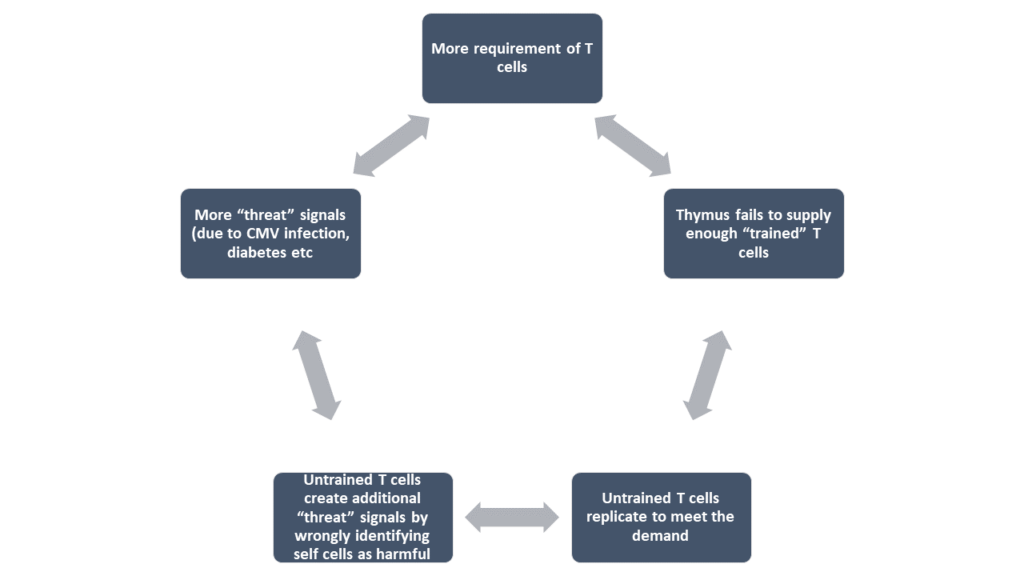
A similar situation can also be accelerated in human body via many other pathological mechanisms. Take, for example, cytomegalovirus (CMV) infection. It’s a virus. And it infects millions of cells very rapidly. It generally doesn’t cause any trouble and tries of coexist without killing the host cells. CMV is quite intelligent in this aspect. It does not cause any deformity in the host cells. Hence, host cells are not destroyed by the immune system. But CMV keeps immune system triggered as it moves from one cell the other. Because of this continuous immune trigger, requirement of new T cells keeps rising. This rising demand for new T cells is bound to soon exhaust the capacity of Thymus to supply trained T cells. Instead, the existing T cells multiply to meet the increasing demand. Again, slowly you will have a growing population of T cells who are not well trained [13].
In short, viral infections (such as CMV) can cause the supply of trained T cells to go down.
Consider a man with uncontrolled diabetes mellitus. The byproducts of circulating sugar keep causing damage along the blood vessel linings. These damages keep happening continuously across miles of blood vessels. Every organ ends up suffering. But this suffering is not just because of the sugar byproducts depositing. The suffering is also because body’s own immune system is attacking these sites. For immune system every “damage” is a “threat” as we noted earlier. How dangerous this immune activation is, in diabetes mellitus, is a matter of another discussion; but the point that is being made is that in diabetes mellitus immune system remains triggered on a continuous basis. And the story repeats: because of this continuous immune trigger, requirement of new T cells keeps rising. This rising demand for new T cells is bound to soon exhaust the capacity of Thymus to supply trained T cells. Instead, the existing T cells multiply to meet the increasing demand. Again, slowly this patient will have a growing population of T cells who are not well trained [14].
Same is true in case of any other such chronic diseases viz. primary hypertension, rheumatoid arthritis etc [15][16].
In short, comorbidities such as diabetes, hypertension, heart disease etc, cause the supply of trained T cells to go down.
Now, let step up- let’s combine all the three stories together- old age + CMV infection + Diabetes/Hypertension. And now you definitely have someone with minimal well-trained T cells; most of the T cells are ill- trained.
You will agree that this is not a rare “someone”. This is nearly everyone around us. By the age of 40 years >50% of population gets infected with CMV [17]. Once CMV infected, you can never get rid of that infection. Diabetes itself has been identified as an epidemic which becomes more common as age advances [18].
But, lets come back to the most important question that must be nagging you (hopefully)- what’s the big deal with not having enough trained T cells?
Trained vs Untrained: The Wrath of Unruly Mercenaries
Remember, we noted that trained T cells are able to differentiate between real threats versus false alarms. The “trained” T cells are able to give focus to the attack unleashed, by specifically targeting the culprits and blunting impact on bystanders- thus minimizing any collateral damage. Once you have majority as “ill- trained” T cells out there in the battlefield the control over innate immunity is lost. Innate immunity doesn’t get the required direction. Plus, now, they get powered by the additional arsenal provided by these “ill trained” T cells. Imagine a troop of mercenaries, not patriotic to any side, armed with powerful weapons with instructions to kill terrorists at all cost. Will they care to differentiate between civilians and terrorists when they fire their weapons?
Now, imagine a 60-year-old man with uncontrolled diabetes mellitus climbing stairs. He is taking support for climbing by grabbing the railings. He has been wearing mask since an hour now, and this mask is now causing some sort of itch under his nose due to accumulated sweat. So, he rubs his fingers against his nose in an attempt to relieve this itch. It is this act which will now trigger a series of unfortunate events.
Few moments ago, a young student had swiped his hand through the same railing. He was fit- no fever, no cold. There was no way for anyone to suspect that he was an asymptomatic carrier of Covid-19.
The virus has now entered the old man’s respiratory tract. It started by entering one cell and hijacking its genetic machinery. Soon, this cell is making multiple copies of the virus. These viruses now in turn infect other cells around. Again, each of these infected cells create multiple copies of this virus. Soon thousands and thousands of cells in the respiratory system are now infected with the virus. Presence of a foreign particle has already triggered the innate immune system. It has started responding. 6 days have gone by. The effects of innate immune system’s activities are now visible. The old man has fever. He is sneezing and coughing. There is slight body ache as well [19]. Innate system has been relentlessly attacking all the cells harboring Covid-19 virus particles. In that, innate immunity has been successful. Adaptive immune system has also joined the fray. Its weapons are much more potent. And here is where things can start going wrong.
An optimally adaptive immune system with “fully trained” T cells would have instructed innate immune system to calm down since its hunting down all the cells which are harboring Covid-19 virus particles. It would have told innate immune system to attack only the virus with minimal impact of self- cells, because these are the same cells that are necessary for functioning of respiratory system. The optimal adaptive immune system itself would have made targeted attacks on the virus and would have spared majority of the self- cells.
But this man is 60 years old. Plus, he has uncontrolled diabetes mellitus. Both these factors have ensured that his immune system is full of “untrained” T cells. Instead of asking the innate immune system to ease down and focus, these untrained T cells reinforce the unrestrained attacks mounted by the innate immune system. The magnitude of this attack maybe measured by testing Interlukin-6 (IL-6) levels at regular intervals. They will be really very high. Same can also be determined by measuring C reactive protein, D- dimer, LDH etc. The cytokine storm is setting in [20].
The wild mercenaries- innate immune system along with “immature” T cells- are wildly spraying bullets on anything that has the virus. Unfortunately, most of the cells of the lungs are harboring this virus. Its Day 8 and oxygen saturation is dropping. X ray will show that more than 50% of lungs is impacted.
By Day 15 cytokine storm reaches its height. Oxygen saturation drops below 70%. Cytokine storm has devoured almost all organs. Liver enzymes are very high indicating massive liver damage. Death is now imminent [21].

Coming Up
In the next part (final part), we will finally try to arrive at a simple scientific way to predict “Who will die in COVID-19?”
Armed with the basic knowledge you gathered in Part 1, Part 2 and this post, the final part will be extremely simple to follow. Hopefully after that, if you see a patient infected with COVID-19 you might have a way to predict if he/she will require hospitalization.
References
[18] “Diabetes.” https://www.who.int/news-room/fact-sheets/detail/diabetes (accessed Apr. 22, 2021).


I have read your article carefully and I agree with you very much. This has provided a great help for my thesis writing, and I will seriously improve it. However, I don’t know much about a certain place. Can you help me?
Thank you for your sharing. I am worried that I lack creative ideas. It is your article that makes me full of hope. Thank you. But, I have a question, can you help me?
Your enticle helped me a lot, is there any more related content? Thanks!
Your article gave me a lot of inspiration, I hope you can explain your point of view in more detail, because I have some doubts, thank you.
Your article gave me a lot of inspiration, I hope you can explain your point of view in more detail, because I have some doubts, thank you. 20bet